
The Ketogenic Diet for PCOS: Should You Try It?
A once little-known therapeutic diet has had a meteoric rise to fame in recent years. It has been touted as a treatment for everything from cancer to, you guessed it, PCOS. Let’s discuss what the ketogenic diet actually is, and how likely it is to help manage PCOS symptoms according to the research.
Key Takeaways
The ketogenic diet is a therapeutic diet that requires extremely low carbohydrate, moderate protein, and high fat intake to achieve ketosis. Getting (and staying) in ketosis requires complete avoidance of carbohydrate-rich foods and careful food tracking.
The majority of studies in this area utilize a very low calorie ketogenic diet (VLCKD), where participants eat 600-800 calories for 4+ weeks (yes, you read that right). VLCKDs are not safe or feasible for the average woman with PCOS, don’t isolate the impact of the ketogenic diet, and lack long-term follow-up periods needed to know if all that pain brought any gain.
The few non-VLCKD studies that exist report reduced weight, triglycerides, insulin levels, and menstrual cycle length after an 8 - 12 week keto diet. The impact on cholesterol, glucose levels, and insulin resistance were conflicting; some studies showed an improvement while others did not.
While the results of these short-term studies may seem impressive at first-look, small sample sizes and flaws in the study design and methodologies call some of the findings into serious question.
The challenges and risks of adopting a ketogenic diet for PCOS are not justified by the research as it stands. Generally, keto is not superior to other calorie-matched diets for weight loss or metabolic improvements long-term, and comes with significant risks.
What is the ketogenic diet?
The purpose of the ketogenic diet is to get into a state of ketosis, which is when the body uses mostly fatty acids and ketones for energy. Normally, carbohydrates (i.e. glucose) are the main energy source. But, when carbohydrate intake is low, most cells can break down fatty acids for energy. Ketone bodies are produced from fat and provide fuel to cells that can’t break down fatty acids directly. We produce fatty acids and ketone bodies to a small degree during intense or extended exercise sessions, and when we sleep.
Making small amounts of ketone bodies is very different from being in ketosis. Getting into ketosis (and staying in it) requires very low intake of carbohydrates to essentially force the body to use alternate fuel sources. We’re talking 20 - 50 grams a day, well below the daily recommended minimum carbohydrate intake of 130 grams.
Carbohydrate-rich foods like whole grains, bread, pasta, beans, milk, most fruits, starchy vegetables (e.g. potatoes, corn), alcohol, juice, and sugar-sweetened desserts and drinks are completely avoided. Protein intake is limited because some amino acids (which make up proteins) can be converted to glucose. Most daily calories come from fat, which can’t be converted into glucose.
And now for some quick myth-busting. A common refrain amongst keto enthusiasts is that it’s superior for weight loss because you use your body’s own fat stores for fuel. It’s true that body fat can be used for energy as free fatty acids or made into ketone bodies, but so can dietary fat (which is consumed in high amounts). When keto diets go toe-to-toe with calorie-matched controls, they are equally as effective for long-term weight loss [1, 2, 3, 4, 5]. And, rapid initial weight loss seen with ketogenic diets is largely due to water loss, not fat loss [5]. Ultimately, you need to be in a calorie deficit to lose weight. That said, ketogenic diets may have a unique advantage for promoting satiety and reducing hunger, making it easier to stay in a calorie deficit and lose weight [6, 7].
The restrictive nature of the ketogenic diet comes with a lot of drawbacks that make it difficult and potentially dangerous to sustain long-term. Cutting out entire food groups can quickly lead to nutrient deficiencies and make navigating social situations with food challenging. Meals must be carefully planned and tracked to ensure carbohydrate levels stay below the strict limit. High fat and potentially lower fiber intake can cause GI discomfort and constipation. Long-term ketogenic diets are associated with increased LDL cholesterol, a major risk factor for heart disease [8]. In mice, long-term ketogenic diets caused high blood lipids, liver dysfunction, and glucose intolerance [9]. Low carbohydrate diets have also been associated with increased risk of mortality when coupled with high animal-derived fat and protein intake [10].
How can keto help with PCOS?
Women with PCOS have been shown to be less sensitive to the effects of insulin; an estimated 60 - 95% of women with PCOS are insulin resistant [11, 12, 13]. Insulin is the hormone that spikes after meals, telling cells to take up glucose. Insulin resistance means that cells have a reduced response to insulin, requiring the pancreas to release more and more insulin to move glucose from the bloodstream into the cell. As insulin resistance progresses, it becomes harder to produce enough insulin to maintain blood glucose levels. Over time, this can lead to high blood sugar.
The relationship between insulin resistance and PCOS is complex and not fully understood, but it is thought to be a significant driver of symptoms in many women with PCOS [14]. Diets that restrict carbohydrates have been proposed as a way to reduce insulin and glucose levels, improve insulin sensitivity, and manage symptoms.
What The Research Tells Us
Very Low Calorie Ketogenic Diets
The published research in this area is fairly limited (shocking, I know). To make matters worse, a lot of studies on the ketogenic diet and PCOS investigate the impact of very low calorie ketogenic diets (VLCKDs). These diets are typically 600 - 800 calories and fewer than 30 grams of carbohydrates per day for 4+ weeks. Unsurprisingly, participants lost a significant amount of weight and saw improvements in insulin sensitivity and lipid levels (e.g., cholesterol). Some studies also reported improved menstrual regularity and reduced androgen levels [15, 16, 17, 18, 19, 20].*
The glaring issue with these studies is that they don’t isolate the impact of the ketogenic diet. So, it’s impossible to say whether improvements were due to the ketogenic diet specifically or the extreme calorie deficit (and significant weight loss that followed). A study that compared an 8-week very low-calorie diet (non-ketogenic) to a moderate calorie deficit in women with PCOS showed similar results to the very low calorie ketogenic diets discussed above, especially for weight loss and glucose control [21]. This suggests that extreme calorie restriction is driving at least some of the results seen in the VLCKD studies.
Also, none of the VLCKD studies included a follow-up period, so we don’t know whether the positive changes lasted after participants returned to their normal diet. Longer-term data from other very low calorie diet studies is also limited, but can provide some insight on weight maintenance specifically. Sustained weight loss in the 1 - 5 years following a very low calorie diet varies a lot [22]. While they produce rapid short-term weight loss, over time the results are similar to weight loss achieved by more moderate calorie deficits, especially when participants lacked long-term support [23, 24].
Since most of the studies on the ketogenic diet for PCOS utilize VLCKDs, this wouldn’t be a comprehensive article without at least touching on them. That said, I do not recommend following a very low calorie diet! In addition to being miserable, there are serious risks that come with eating way below your body’s energy needs for weeks at a time such as dehydration, electrolyte imbalances (which can be fatal), nutrient deficiencies, gallstones, and the potential to develop disordered eating habits. Loss of muscle mass is a significant risk of very low calorie diets and has countless negative health impacts, including reducing your metabolic rate, which can make weight management harder long-term.
Now let’s dive into studies that reflect a more realistic approach to better understand how the ketogenic diet impacts body composition, metabolic health, menstrual regularity, and reproductive hormones in women with PCOS.
Body Composition
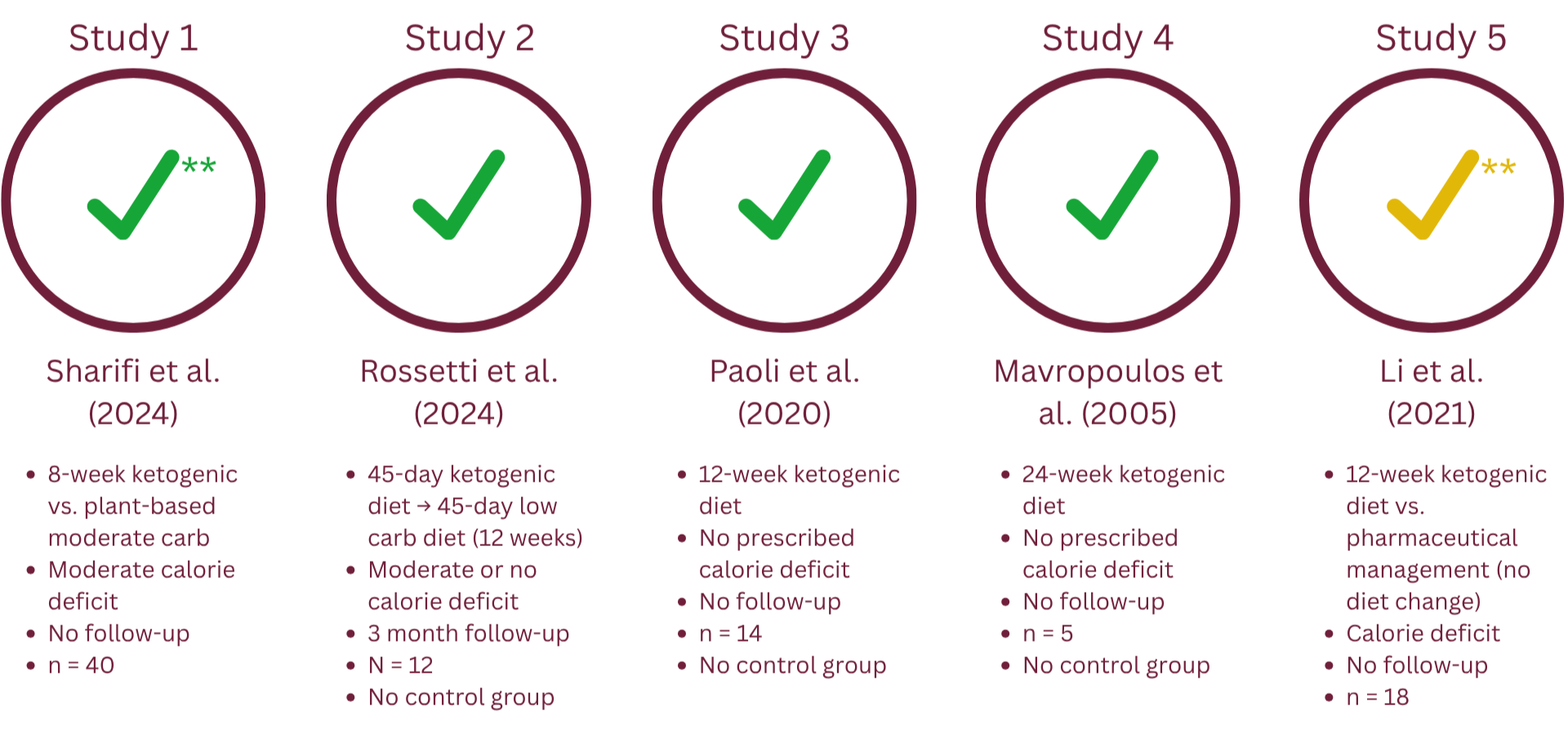
Summary body composition findings by study
Most studies reported a statistically significant reduction in body weight and BMI, which is expected given that participants were frequently placed in a moderate kcal deficit [25, 26, 27, 28, 29]. Beyond weight and BMI, all studies that tracked hip and waist circumference, fat mass, and visceral fat generally reported a significant decrease across all metrics [25, 26, 27, 29].** Visceral fat is a type of fat that surrounds your internal organs and is a risk factor for type 2 diabetes and heart disease, among other things. In Li et al., the ketogenic group’s weight loss and reduction in BMI, fat mass, and visceral fat lost significance when compared to the control group, meaning the ketogenic diet didn’t show a demonstrated treatment effect [29].
Only one study by Sharifi et al. included a control group that kept calories consistent between the control and ketogenic diet group. In this study, the ketogenic diet group ate in a moderate calorie deficit and consumed fewer than 30 grams of carbs daily. The “control” group ate a vegan moderate carbohydrate diet that was the same number of calories [25].
Both groups in Sharifi et al. saw an improvement in weight, waist circumference, and hip circumference, but the ketogenic diet performed better than the control group, especially on waist and hip circumference [25]. While the keto group lost more weight, the difference in the average weight loss between groups was only 2.8 lbs, a statistically significant but fairly small difference. Both groups lost a similar amount of visceral fat [25]. The ketogenic diet group lost more body fat, but had a greater reduction in lean body mass (also called fat free mass) as a percentage of overall weight loss [25]. While ketogenic diets tend to lead to greater loss of fat free mass than calorie-matched diets, a recent meta-analysis found that ketogenic diets did not have a negative impact on muscle mass, power, or strength compared to controls [30]. Loss of lean body mass is likely due to reduced water and glycogen (stored glucose) in the muscle, not muscle mass.
These findings are in alignment with the general understanding that ketogenic diets promote weight loss. The specific effects of the ketogenic diet on body composition such as fat mass, fat free mass, and visceral fat compared to other eating patterns are less certain, as the only two controlled studies (Li et al. and Sharifi et al.) measured body composition using bioelectrical impedance (BIA), an unreliable method.**
Metabolic Health
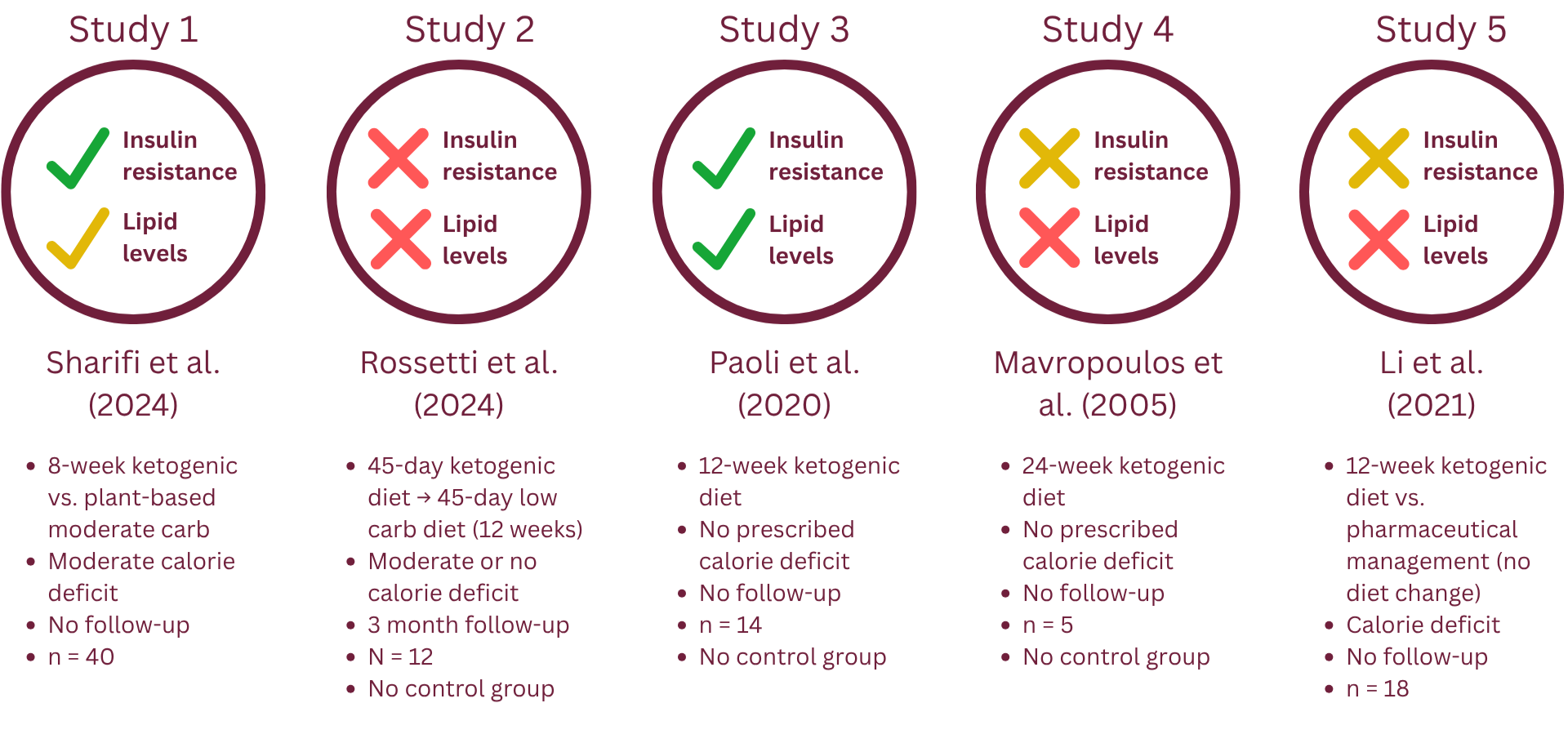
Summary metabolic health findings by study
When it comes to glucose control and insulin resistance (measured as HOMA-IR), the results are conflicting.
Two studies reported a statistically significant reduction in insulin resistance and fasting glucose [25, 27]. Another study found no significant change in HOMA-IR or fasting glucose levels [26]. Two studies that reported on fasting glucose (but not insulin resistance) reported no significant change [28, 29]. In Sharifi et al., the keto group had a greater decrease in HOMA-IR, glucose, and insulin than the control group, although both groups saw significant improvements [25]. Insulin levels dropped significantly across the board [25, 26, 27, 28]. This is expected after transitioning to a low-carbohydrate diet because carbohydrates generally cause insulin to rise more compared to protein and fat, but there could be another explanation (more below).
Two studies found that the ketogenic diet improved lipid parameters by lowering triglycerides, total cholesterol and LDL cholesterol as well as increasing HDL cholesterol [25, 27]. Another found that the ketogenic diet only improved HDL cholesterol, without any change in total or LDL cholesterol [26]. In Sharifi et al., both the ketogenic and “control” plant-based group improved their lipid profiles, but the plant-based group lowered total cholesterol and LDL cholesterol and increased HDL cholesterol more than the keto group [25]. The two remaining studies found no statistically significant change in lipid levels [28, 29].
Li et al. compared the effects of a 3-month ketogenic diet to pharmaceutical management of liver dysfunction in women with PCOS [29]. The ketogenic diet group showed significantly improved liver function compared to the control group at the end of the intervention. This small study agrees with research on the general population showing that short-term ketogenic diets are effective in treating early-stage fatty liver, but more information on safety is needed [31, 32].
Although one of the main benefits of the ketogenic diet is thought to be improved glucose control and insulin resistance, that is not consistently shown here. Although many participants were insulin resistant, their glucose levels were still normal. In these cases, reduced insulin levels may suggest improved insulin sensitivity without a significant change in HOMA-IR. However, we don’t have enough information about the participants to know if this is the case. If you’re looking to improve lipid levels, the ketogenic diet may not be the best choice, especially compared to a more plant-based eating pattern.
Menstrual Cycle Length and Regularity
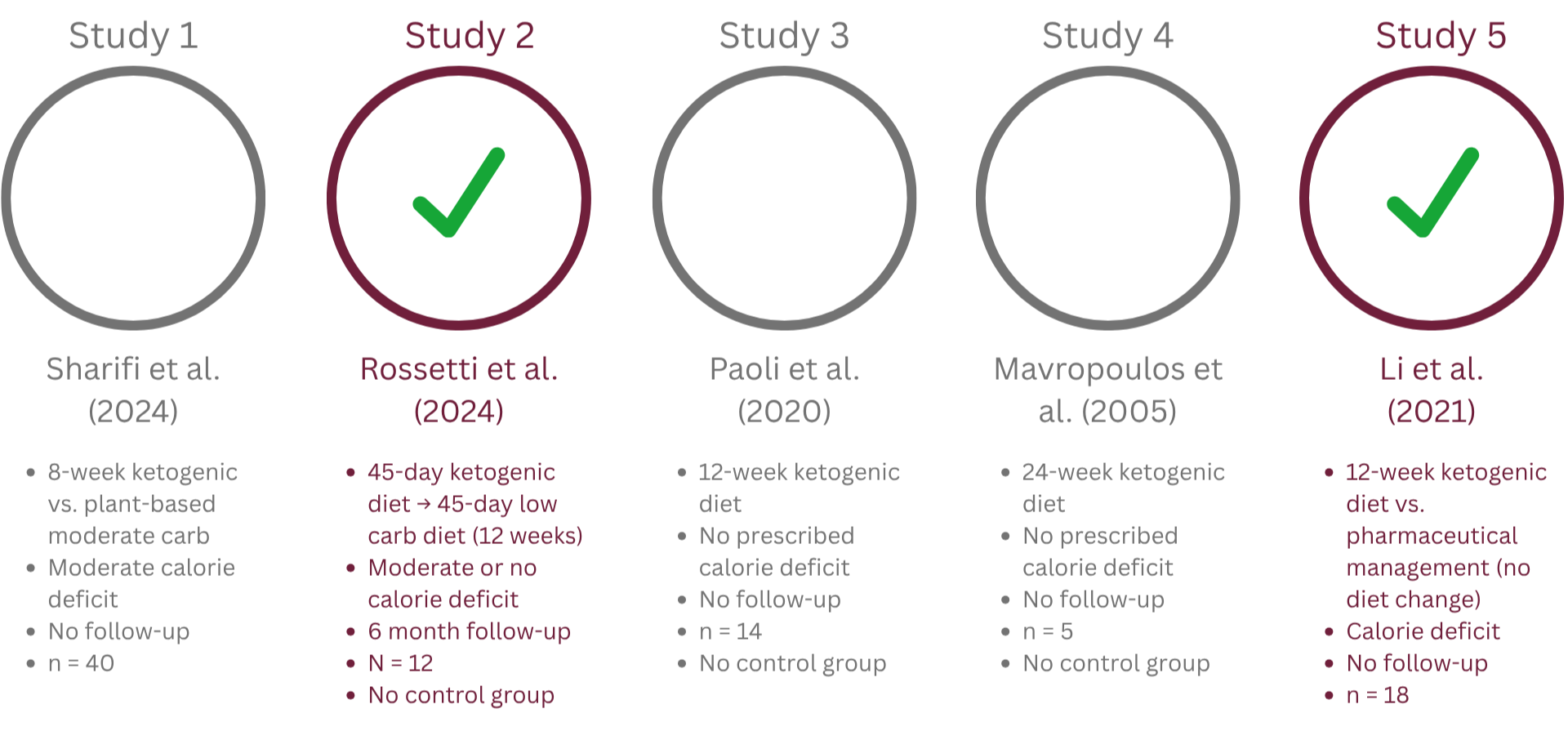
Summary cycle length findings by study
Only two studies tracked menstrual regularity. In Rossetti et al., at the end of the 6-month follow-up period (3 months after diet completion), all 12 participants reported improved menstrual cycle regularity, with the median cycle length decreasing from 47.5 to 32 days [26]. Li et al. observed a statistically significant reduction in menstrual cycle length in the ketogenic diet group, from 72.5 to 32.5 days. Improvements in cycle length were not significantly different between the keto and control group, which was placed on a hormonal contraceptive to regulate cycle length [29].
While small, these studies delivered impressive results with regard to cycle length. However, participants also lost weight. Since even modest weight loss of 2-5% has been shown to shorten cycle length and restore ovulation in women with PCOS, it’s possible that the weight loss and not the ketogenic diet explains these results [33, 34, 35].
Reproductive Hormones
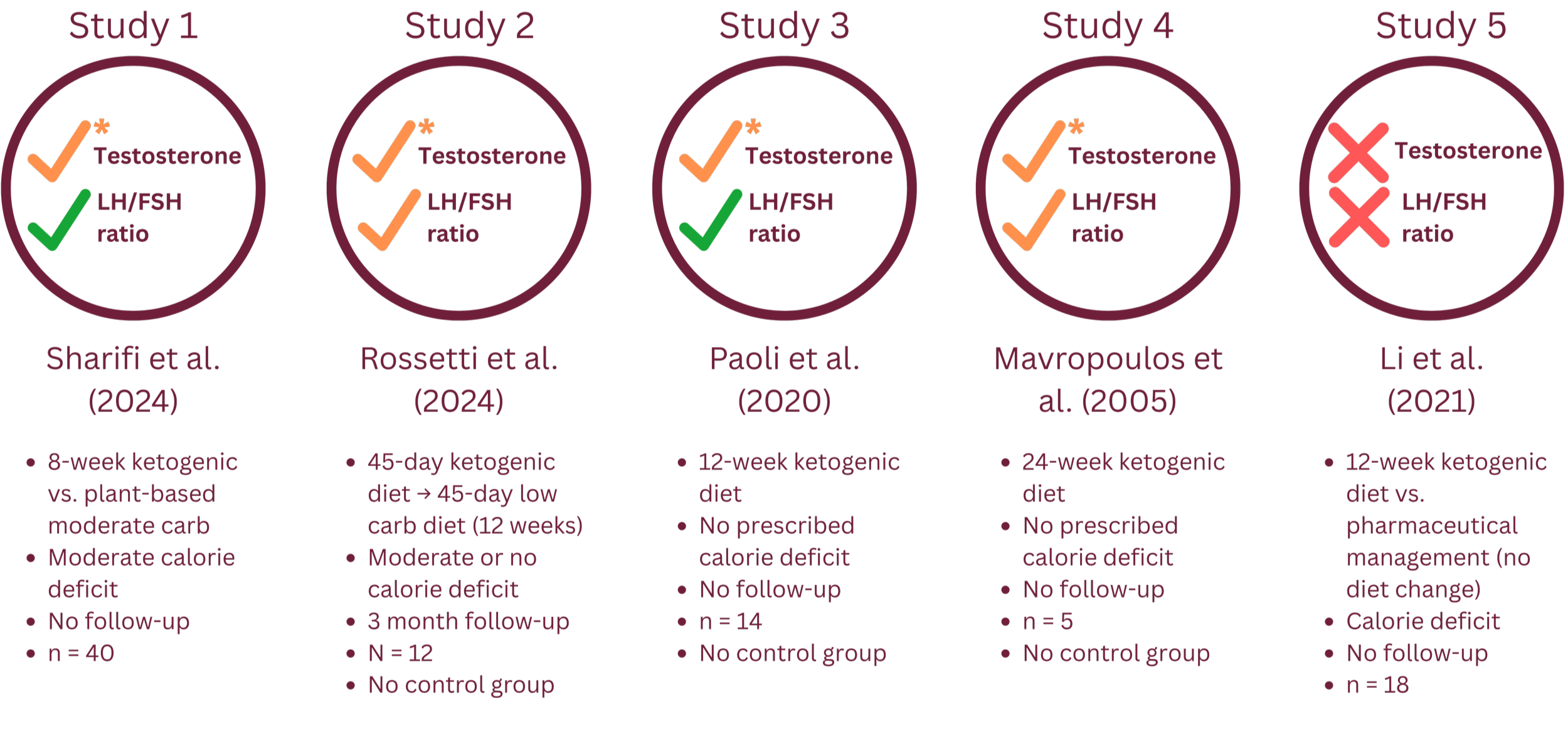
Summary reproductive hormone findings by study
All but one study found a statistically significant reduction in testosterone levels. However, all of these studies used a method to measure testosterone that is notoriously inaccurate in women and has been recommended against for decades.* So, these studies do not provide strong enough evidence to say that keto reduces testosterone levels. High testosterone can show up in other ways, too. For example, hair growth (hirsutism) is a known symptom of high testosterone and is measured by the Ferriman-Gallwey score (mFG). Three studies tracked mFG; two found no change and one did [25, 26, 27].
Four studies tracked changes in follicle-stimulating hormone (FSH) and luteinizing hormone (LH). LH and FSH are usually in a 1:1 ratio; in PCOS this ratio can sometimes be 2:1 or higher. LH and FSH levels fluctuate throughout the menstrual cycle, so they need to be measured on cycle day 2, 3, 4, or 5 for the most accurate result. By this point you can probably already see where I’m going with this one: that didn’t always happen. Two studies reported an improved LH/FSH ratio but did not specify the cycle day [26, 28]. The other two studies measured within an acceptable window and found an improved LH/FSH ratio [25, 27].
One study also reported increased sex-hormone binding globulin (SHBG) levels [27]. SHBG is a protein made in the liver that binds to and “inactivates” testosterone (and other sex hormones) as it travels through the bloodstream. SHBG tends to be lower in PCOS, which can worsen symptoms because a greater percentage of testosterone is free in the blood and can act on tissues.
Although these results may seem promising, the lack of rigor around proper testing around testosterone and LH/FSH levels makes them pretty unreliable. The jury is still out on this one.
Summing it All Up
Most of the (very few) studies on the ketogenic diet and PCOS consistently reported significant reductions in weight, triglycerides, insulin levels, and menstrual cycle length. There were conflicting results for glucose, HOMA-IR (a measure of insulin resistance), and cholesterol; some studies showed improvement while others did not.
All studies had significant design and methodological flaws that could have impacted the results. For example, most did not include a control group, which makes it difficult to assess whether the ketogenic diet is uniquely beneficial for those with PCOS compared to other dietary approaches. In addition, using inaccurate tools to measure body composition and hormone levels means those results could be incorrect. Most of the studies did not include a follow-up period beyond the diet intervention to assess whether the benefits were maintained long-term. And, while not necessarily a flaw, the sample sizes were quite small and often focused on participants with a BMI > 25, so the wider applicability is unknown.
In my opinion, the challenges and risks of adopting a ketogenic diet are not yet justified by the research as it stands. A number of different dietary approaches have been shown to be effective for managing PCOS; the best eating pattern is going to be the one that is most realistic, sustainable, and tailored to your health goals. Long-term ketogenic diets pose significant health risks, but in the short-term (1 - 3 month) are generally safe for most people.*** If you’re interested in giving it a try, don’t go it alone! A registered dietitian can help you get started on a ketogenic diet, and guide you through reintroducing carbohydrates and maintaining results long-term.
Got a question, comment, or keto diet success or fail? Let me know in the comments below.
*Testosterone levels are highest in the morning and should be measured before 10am. Immunoassays are the most common method for measuring testosterone, but they are notoriously inaccurate in women who have lower testosterone levels and require a more sensitive testing method. Liquid chromatography-tandem mass spectrometry (LC-MS/MS) provides the most accurate results and is considered the gold standard for measuring testosterone in women.
**Dual-Energy X-ray Absorptiometry (DEXA) is the gold-standard for measuring body composition (fat mass, fat free/lean body mass, and visceral fat). Bioelectrical impedance analysis (BIA) is faster and more cost-effective, but is not nearly as accurate as DEXA. Half of the studies mentioned used DEXA, and half used BIA. The takeaways from BIA and DEXA generally agreed, which is why I included the BIA findings here.
***Ketogenic diets are not recommended for anyone with type 1 diabetes, severe liver disease, gallbladder disease, pancreatic disease, kidney disease, those on SGLT-2 inhibitors for the treatment of type 2 diabetes, a history of eating disorders, or those who are pregnant or breastfeeding.